Client intake form Inner Harmony (PDF)
File information
Title: Microsoft Word - Client intake form_Inner Harmony.docx
Author: Rebecca Melaragno
This PDF 1.3 document has been generated by Word / Mac OS X 10.7.5 Quartz PDFContext, and has been sent on pdf-archive.com on 21/08/2015 at 00:29, from IP address 104.246.x.x.
The current document download page has been viewed 468 times.
File size: 79.31 KB (1 page).
Privacy: public file
File preview
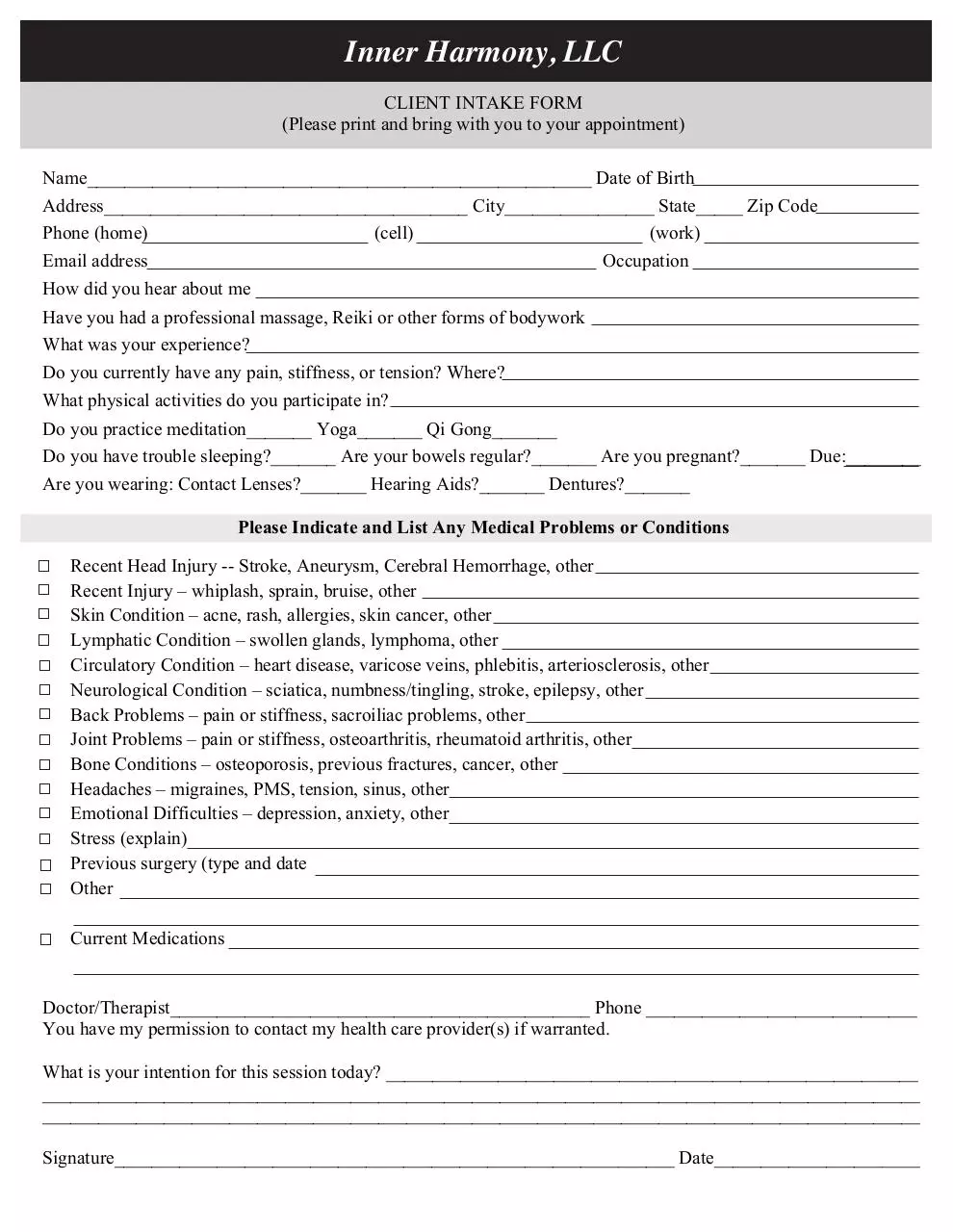
Inner Harmony, LLC
CLIENT INTAKE FORM
(Please print and bring with you to your appointment)
Name______________________________________________________ Date of Birth
Address_______________________________________ City________________ State_____ Zip Code
Phone (home)
(cell)
(work)
Email address
Occupation
How did you hear about me
Have you had a professional massage, Reiki or other forms of bodywork
What was your experience?
Do you currently have any pain, stiffness, or tension? Where?
What physical activities do you participate in?
Do you practice meditation_______ Yoga_______ Qi Gong_______
Do you have trouble sleeping?_______ Are your bowels regular?_______ Are you pregnant?_______ Due:________
Are you wearing: Contact Lenses?_______ Hearing Aids?_______ Dentures?_______
Please Indicate and List Any Medical Problems or Conditions
Recent Head Injury -- Stroke, Aneurysm, Cerebral Hemorrhage, other
Recent Injury – whiplash, sprain, bruise, other
Skin Condition – acne, rash, allergies, skin cancer, other
Lymphatic Condition – swollen glands, lymphoma, other
Circulatory Condition – heart disease, varicose veins, phlebitis, arteriosclerosis, other
Neurological Condition – sciatica, numbness/tingling, stroke, epilepsy, other
Back Problems – pain or stiffness, sacroiliac problems, other
Joint Problems – pain or stiffness, osteoarthritis, rheumatoid arthritis, other
Bone Conditions – osteoporosis, previous fractures, cancer, other
Headaches – migraines, PMS, tension, sinus, other
Emotional Difficulties – depression, anxiety, other
Stress (explain)
Previous surgery (type and date
Other
Current Medications
Doctor/Therapist_____________________________________________ Phone _____________________________
You have my permission to contact my health care provider(s) if warranted.
What is your intention for this session today? _________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
Signature____________________________________________________________ Date______________________
Download Client intake form Inner Harmony
Client intake form_Inner Harmony.pdf (PDF, 79.31 KB)
Download PDF
Share this file on social networks
Link to this page
Permanent link
Use the permanent link to the download page to share your document on Facebook, Twitter, LinkedIn, or directly with a contact by e-Mail, Messenger, Whatsapp, Line..
Short link
Use the short link to share your document on Twitter or by text message (SMS)
HTML Code
Copy the following HTML code to share your document on a Website or Blog
QR Code to this page

This file has been shared publicly by a user of PDF Archive.
Document ID: 0000296942.