PHI HIPAA Acknowledgement 2015 (PDF)
File information
This PDF 1.7 document has been generated by / Foxit PhantomPDF Printer Version 6.0.4.1129, and has been sent on pdf-archive.com on 15/02/2016 at 17:47, from IP address 73.247.x.x.
The current document download page has been viewed 378 times.
File size: 58.75 KB (1 page).
Privacy: public file
File preview
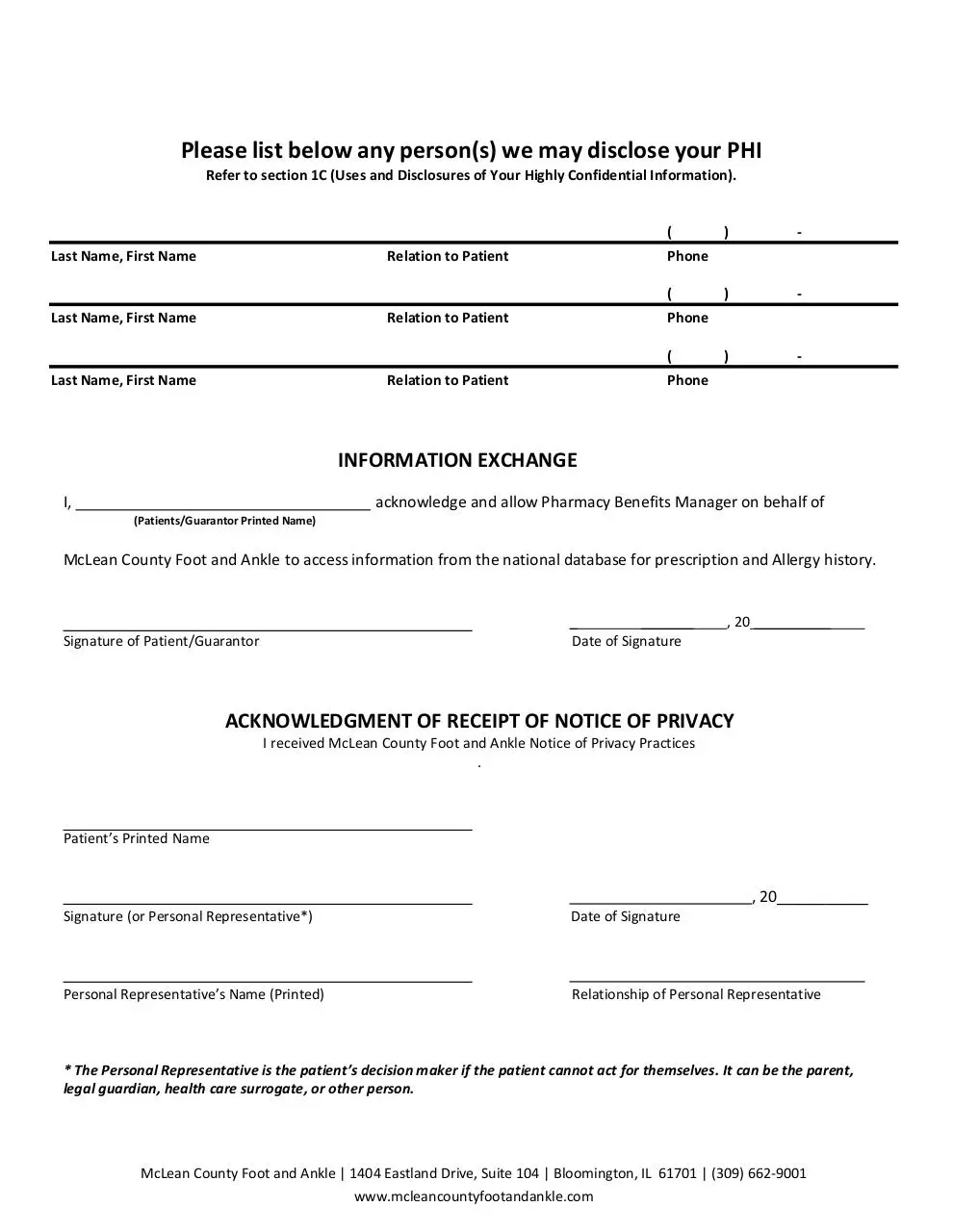
Please list below any person(s) we may disclose your PHI
Refer to section 1C (Uses and Disclosures of Your Highly Confidential Information).
(
Last Name, First Name
Relation to Patient
(
Last Name, First Name
Relation to Patient
-
)
-
)
-
Phone
(
Last Name, First Name
)
Phone
Relation to Patient
Phone
INFORMATION EXCHANGE
I,
acknowledge and allow Pharmacy Benefits Manager on behalf of
(Patients/Guarantor Printed Name)
McLean County Foot and Ankle to access information from the national database for prescription and Allergy history.
_
_______
Date of Signature
Signature of Patient/Guarantor
, 20 __________
ACKNOWLEDGMENT OF RECEIPT OF NOTICE OF PRIVACY
I received McLean County Foot and Ankle Notice of Privacy Practices
.
Patient’s Printed Name
, 20___________
Signature (or Personal Representative*)
Date of Signature
Personal Representative’s Name (Printed)
Relationship of Personal Representative
* The Personal Representative is the patient’s decision maker if the patient cannot act for themselves. It can be the parent,
legal guardian, health care surrogate, or other person.
McLean County Foot and Ankle | 1404 Eastland Drive, Suite 104 | Bloomington, IL 61701 | (309) 662-9001
www.mcleancountyfootandankle.com
Download PHI HIPAA Acknowledgement 2015
PHI HIPAA Acknowledgement 2015.pdf (PDF, 58.75 KB)
Download PDF
Share this file on social networks
Link to this page
Permanent link
Use the permanent link to the download page to share your document on Facebook, Twitter, LinkedIn, or directly with a contact by e-Mail, Messenger, Whatsapp, Line..
Short link
Use the short link to share your document on Twitter or by text message (SMS)
HTML Code
Copy the following HTML code to share your document on a Website or Blog
QR Code to this page
This file has been shared publicly by a user of PDF Archive.
Document ID: 0000340150.