C4 Roventure Time (PDF)
File information
This PDF 1.7 document has been generated by PScript5.dll Version 5.2.2 / Acrobat Distiller 9.0.0 (Windows), and has been sent on pdf-archive.com on 07/03/2016 at 14:27, from IP address 121.222.x.x.
The current document download page has been viewed 272 times.
File size: 126.91 KB (1 page).
Privacy: public file
File preview
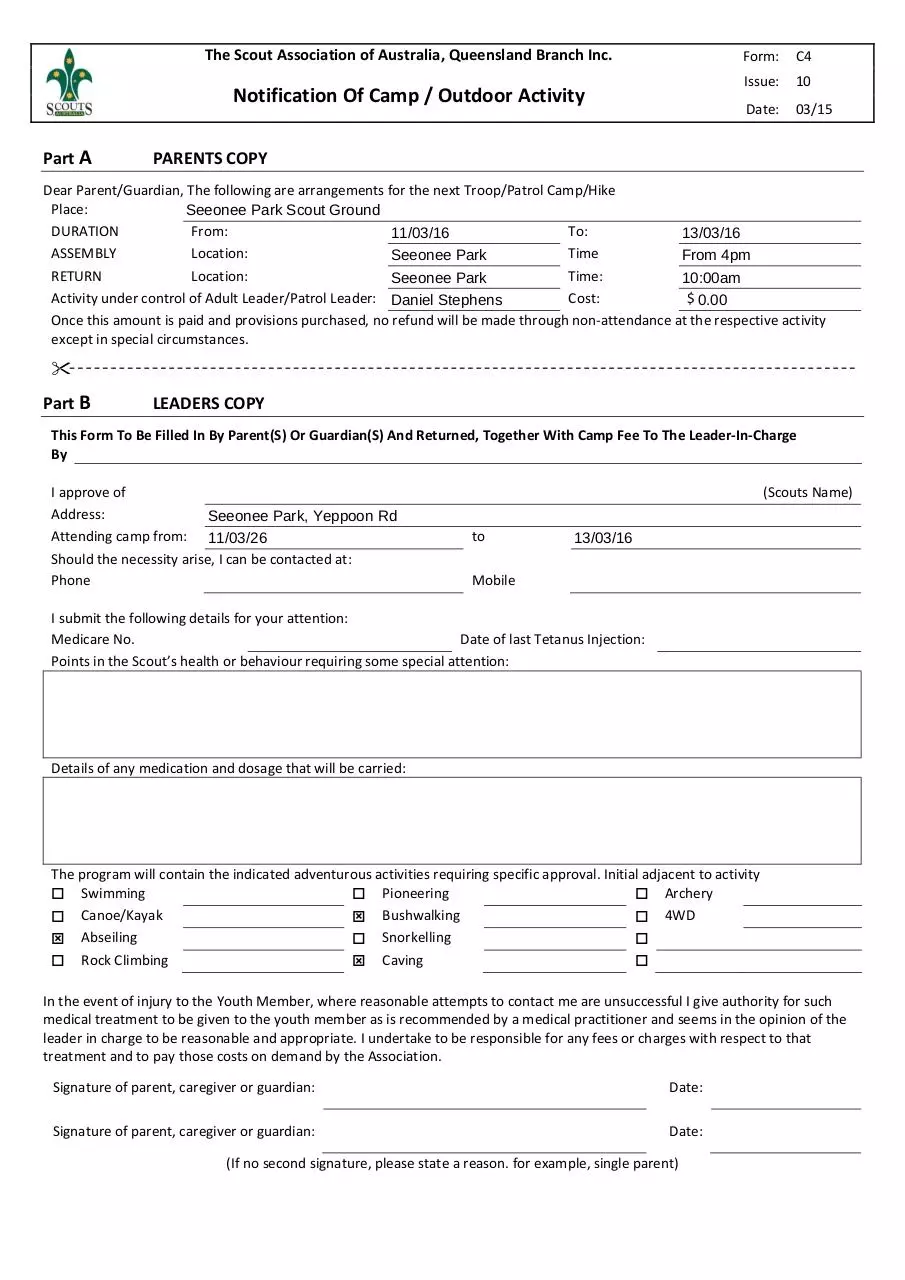
The Scout Association of Australia, Queensland Branch Inc.
Form: C4
Issue: 10
Notification Of Camp / Outdoor Activity
Date: 03/15
Part A
PARENTS COPY
Dear Parent/Guardian, The following are arrangements for the next Troop/Patrol Camp/Hike
Place:
Seeonee
Park Scout Ground
DURATION
From:
To:
11/03/16
13/03/16
ASSEMBLY
Location:
Time
Seeonee Park
From
4pm
RETURN
Location:
Time:
Seeonee Park
10:00am
Activity under control of Adult Leader/Patrol Leader: Daniel Stephens
Cost:
$ 0.00
Once this amount is paid and provisions purchased, no refund will be made through non‐attendance at the respective activity
except in special circumstances.
Part B
LEADERS COPY
This Form To Be Filled In By Parent(S) Or Guardian(S) And Returned, Together With Camp Fee To The Leader‐In‐Charge
By
I approve of
Address:
Seeonee
Park, Yeppoon Rd
Attending camp from: 11/03/26
Should the necessity arise, I can be contacted at:
Phone
(Scouts Name)
to
13/03/16
Mobile
I submit the following details for your attention:
Medicare No.
Date of last Tetanus Injection:
Points in the Scout’s health or behaviour requiring some special attention:
Details of any medication and dosage that will be carried:
The program will contain the indicated adventurous activities requiring specific approval. Initial adjacent to activity
Swimming
Pioneering
Archery
Canoe/Kayak
Bushwalking
4WD
Abseiling
Snorkelling
Rock Climbing
Caving
In the event of injury to the Youth Member, where reasonable attempts to contact me are unsuccessful I give authority for such
medical treatment to be given to the youth member as is recommended by a medical practitioner and seems in the opinion of the
leader in charge to be reasonable and appropriate. I undertake to be responsible for any fees or charges with respect to that
treatment and to pay those costs on demand by the Association.
Signature of parent, caregiver or guardian:
Date:
Signature of parent, caregiver or guardian:
Date:
(If no second signature, please state a reason. for example, single parent)
Download C4 - Roventure Time
C4 - Roventure Time.pdf (PDF, 126.91 KB)
Download PDF
Share this file on social networks
Link to this page
Permanent link
Use the permanent link to the download page to share your document on Facebook, Twitter, LinkedIn, or directly with a contact by e-Mail, Messenger, Whatsapp, Line..
Short link
Use the short link to share your document on Twitter or by text message (SMS)
HTML Code
Copy the following HTML code to share your document on a Website or Blog
QR Code to this page

This file has been shared publicly by a user of PDF Archive.
Document ID: 0000347248.