CCM agreement and consent form (PDF)
File information
Author: Lewis, Kathryn
This PDF 1.5 document has been generated by Microsoft® Word 2016, and has been sent on pdf-archive.com on 30/11/2016 at 07:01, from IP address 75.174.x.x.
The current document download page has been viewed 715 times.
File size: 479.75 KB (2 pages).
Privacy: public file

File preview
Practice
1234 Anywhere Street
Sunny, CA
January 1, 2015
Dear Patients and Families of Practice,
We are pleased to announce that our medical practice, which cares for people with multiple chronic
conditions, will be participating in the Centers for Medicare and Medicaid Services new Chronic Care
Management (CCM) Initiative. Medicare is promoting this concept due to the high morbidity and
spending associated with caring for those with multiple conditions with the expectation that additional
reimbursement to practices focused on care management will help improve quality and reduce health
care costs to patients and to Medicare.
CCM will further enable us to provide the best possible care to our patients, by expanding our
capabilities. Specifically, it will provide a monthly payment of approximately $42 to practices that
perform CCM to facilitate development of a regularly updated, comprehensive plan of care, enhanced
team-based staffing, and investment in technology.
Standard Medicare Part B payment terms apply to CCM, just as any other Part B service. Because of the
nature of our practice and our adoption of a systematic care management program, enrollment is
strongly encouraged for all patients who qualify for CCM (we expect most of our 65+ patients to qualify).
To ensure continued high quality care, please complete the attached consent for CCM services. Patients
or responsible parties, please sign on Page 2 and return to practice manager, by mail, fax or email.
We remain deeply dedicated to providing the best possible care to our patients, and are looking forward
to the additional capabilities CCM will provide us to help us carry out our mission.
Sincerely,
Practice
1234 Anywhere Street
Sunny, CA
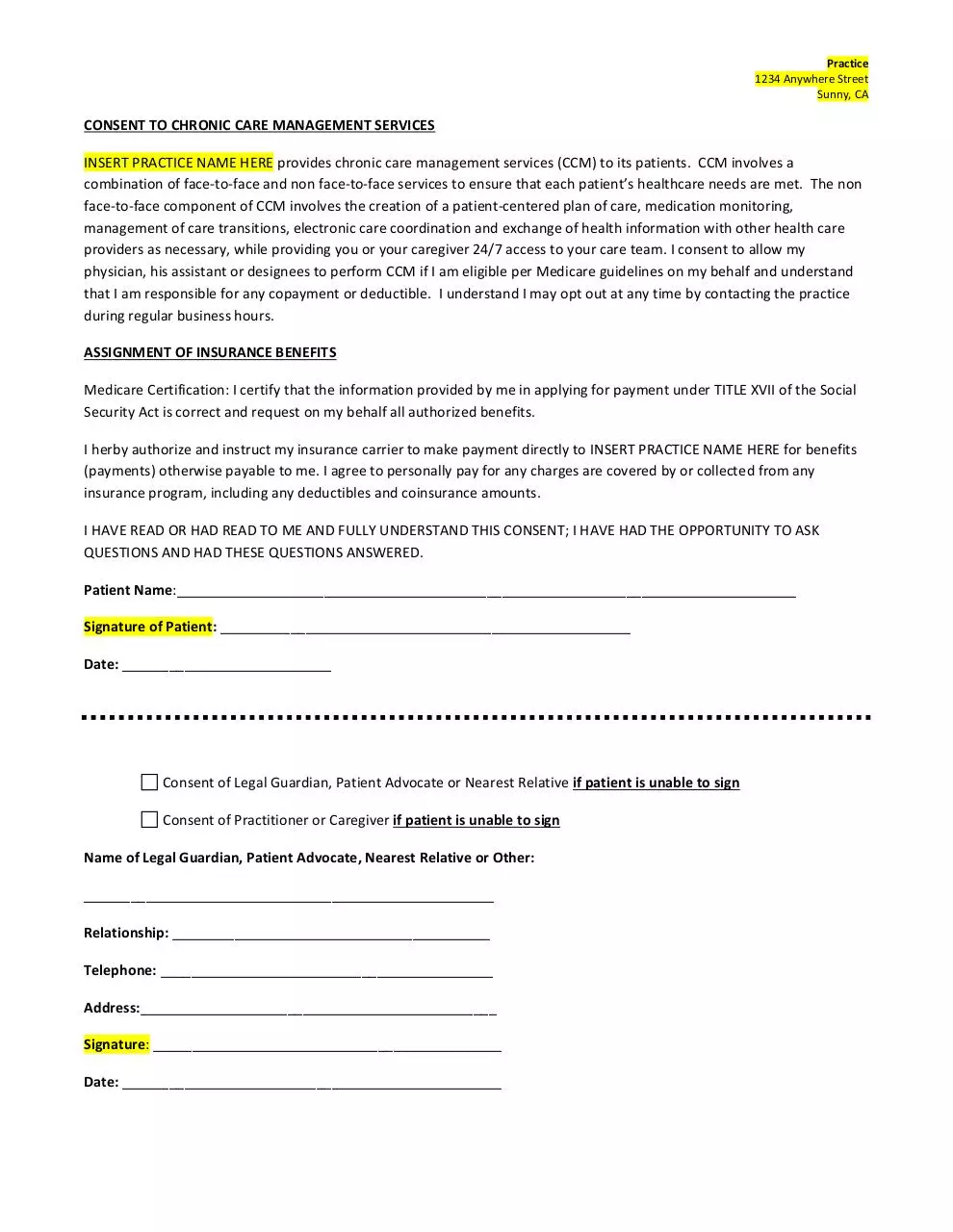
CONSENT TO CHRONIC CARE MANAGEMENT SERVICES
INSERT PRACTICE NAME HERE provides chronic care management services (CCM) to its patients. CCM involves a
combination of face-to-face and non face-to-face services to ensure that each patient’s healthcare needs are met. The non
face-to-face component of CCM involves the creation of a patient-centered plan of care, medication monitoring,
management of care transitions, electronic care coordination and exchange of health information with other health care
providers as necessary, while providing you or your caregiver 24/7 access to your care team. I consent to allow my
physician, his assistant or designees to perform CCM if I am eligible per Medicare guidelines on my behalf and understand
that I am responsible for any copayment or deductible. I understand I may opt out at any time by contacting the practice
during regular business hours.
ASSIGNMENT OF INSURANCE BENEFITS
Medicare Certification: I certify that the information provided by me in applying for payment under TITLE XVII of the Social
Security Act is correct and request on my behalf all authorized benefits.
I herby authorize and instruct my insurance carrier to make payment directly to INSERT PRACTICE NAME HERE for benefits
(payments) otherwise payable to me. I agree to personally pay for any charges are covered by or collected from any
insurance program, including any deductibles and coinsurance amounts.
I HAVE READ OR HAD READ TO ME AND FULLY UNDERSTAND THIS CONSENT; I HAVE HAD THE OPPORTUNITY TO ASK
QUESTIONS AND HAD THESE QUESTIONS ANSWERED.
Patient Name:________________________________________________________________________________
Signature of Patient: _____________________________________________________
Date: ___________________________
Consent of Legal Guardian, Patient Advocate or Nearest Relative if patient is unable to sign
Consent of Practitioner or Caregiver if patient is unable to sign
Name of Legal Guardian, Patient Advocate, Nearest Relative or Other:
_____________________________________________________
Relationship: _________________________________________
Telephone: ___________________________________________
Address:______________________________________________
Signature: _____________________________________________
Date: _________________________________________________
Download CCM agreement and consent form
CCM agreement and consent form.pdf (PDF, 479.75 KB)
Download PDF
Share this file on social networks
Link to this page
Permanent link
Use the permanent link to the download page to share your document on Facebook, Twitter, LinkedIn, or directly with a contact by e-Mail, Messenger, Whatsapp, Line..
Short link
Use the short link to share your document on Twitter or by text message (SMS)
HTML Code
Copy the following HTML code to share your document on a Website or Blog
QR Code to this page
This file has been shared publicly by a user of PDF Archive.
Document ID: 0000514775.