TFE WELCOME TO OUR OFFICE (PDF)
File information
Title: NAME:
Author: Valued Gateway Client
This PDF 1.5 document has been generated by Microsoft® Word 2010, and has been sent on pdf-archive.com on 25/09/2017 at 21:30, from IP address 76.108.x.x.
The current document download page has been viewed 143 times.
File size: 95.42 KB (1 page).
Privacy: public file
File preview
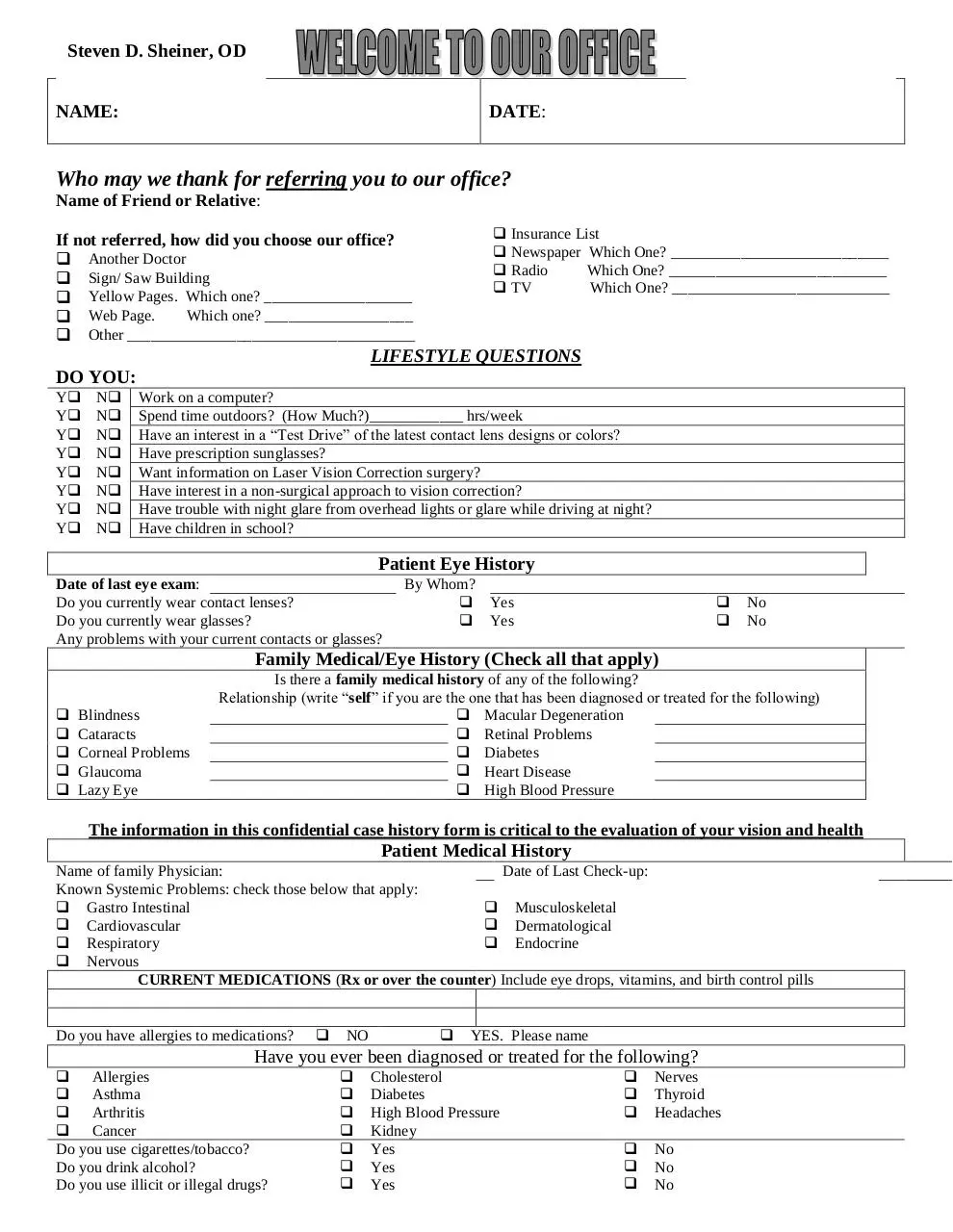
Steven D. Sheiner, OD
DATE:
NAME:
Who may we thank for referring you to our office?
Insurance List
Newspaper Which One? ____________________________
Radio
Which One? ____________________________
TV
Which One? ____________________________
Name of Friend or Relative:
If not referred, how did you choose our office?
Another Doctor
Sign/ Saw Building
Yellow Pages. Which one? ___________________
Which one? ___________________
Web Page.
Other _____________________________________
LIFESTYLE QUESTIONS
DO YOU:
YN
YN
YN
YN
YN
YN
YN
YN
Work on a computer?
Spend time outdoors? (How Much?)____________ hrs/week
Have an interest in a “Test Drive” of the latest contact lens designs or colors?
Have prescription sunglasses?
Want information on Laser Vision Correction surgery?
Have interest in a non-surgical approach to vision correction?
Have trouble with night glare from overhead lights or glare while driving at night?
Have children in school?
Patient Eye History
Date of last eye exam:
Do you currently wear contact lenses?
Do you currently wear glasses?
Any problems with your current contacts or glasses?
By Whom?
Yes
Yes
No
No
Family Medical/Eye History (Check all that apply)
Blindness
Cataracts
Corneal Problems
Glaucoma
Lazy Eye
Is there a family medical history of any of the following?
Relationship (write “self” if you are the one that has been diagnosed or treated for the following)
Macular Degeneration
Retinal Problems
Diabetes
Heart Disease
High Blood Pressure
The information in this confidential case history form is critical to the evaluation of your vision and health
Patient Medical History
Name of family Physician:
Date of Last Check-up:
Known Systemic Problems: check those below that apply:
Gastro Intestinal
Musculoskeletal
Cardiovascular
Dermatological
Respiratory
Endocrine
Nervous
CURRENT MEDICATIONS (Rx or over the counter) Include eye drops, vitamins, and birth control pills
Do you have allergies to medications?
NO
YES. Please name
Have you ever been diagnosed or treated for the following?
Allergies
Asthma
Arthritis
Cancer
Do you use cigarettes/tobacco?
Do you drink alcohol?
Do you use illicit or illegal drugs?
Cholesterol
Diabetes
High Blood Pressure
Kidney
Yes
Yes
Yes
Nerves
Thyroid
Headaches
No
No
No
Download TFE WELCOME TO OUR OFFICE
TFE_WELCOME_TO_OUR_OFFICE.pdf (PDF, 95.42 KB)
Download PDF
Share this file on social networks
Link to this page
Permanent link
Use the permanent link to the download page to share your document on Facebook, Twitter, LinkedIn, or directly with a contact by e-Mail, Messenger, Whatsapp, Line..
Short link
Use the short link to share your document on Twitter or by text message (SMS)
HTML Code
Copy the following HTML code to share your document on a Website or Blog
QR Code to this page

This file has been shared publicly by a user of PDF Archive.
Document ID: 0000677905.