policy change form (PDF)
File information
Author: Musille, Russ
This PDF 1.6 document has been generated by Microsoft® Word 2010, and has been sent on pdf-archive.com on 19/05/2017 at 01:08, from IP address 172.90.x.x.
The current document download page has been viewed 294 times.
File size: 192.59 KB (1 page).
Privacy: public file
File preview
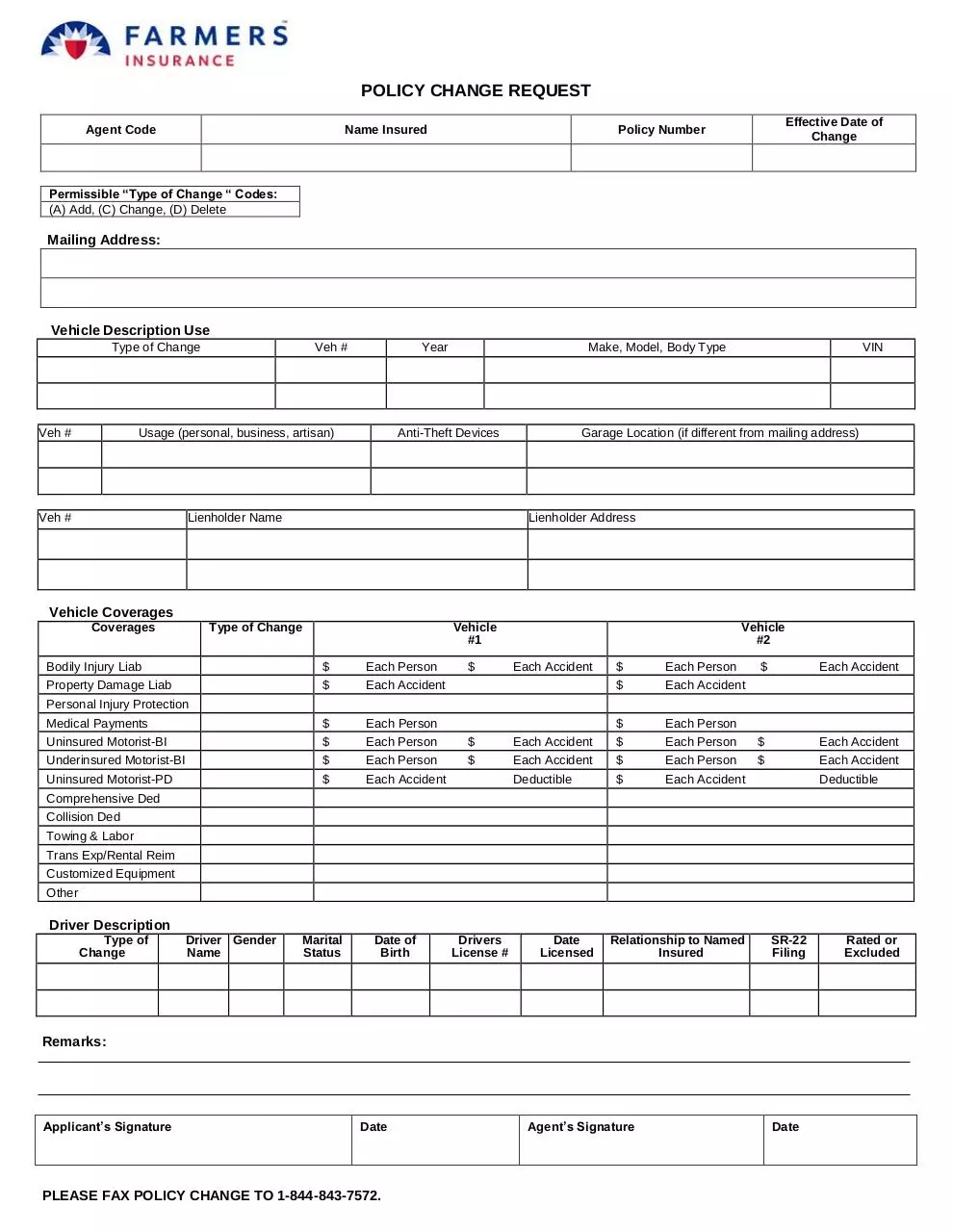
POLICY CHANGE REQUEST
Agent Code
Name Insured
Effective Date of
Change
Policy Number
Permissible “Type of Change “ Codes:
(A) Add, (C) Change, (D) Delete
Mailing Address:
Vehicle Description Use
Type of Change
Veh #
Veh #
Usage (personal, business, artisan)
Veh #
Lienholder Name
Year
Make, Model, Body Type
Anti-Theft Devices
VIN
Garage Location (if different from mailing address)
Lienholder Address
Vehicle Coverages
Coverages
Type of Change
Vehicle
#1
Bodily Injury Liab
$
Each Person
Property Damage Liab
$
Each Accident
Medical Payments
$
Each Person
Uninsured Motorist-BI
Underinsured Motorist-BI
$
$
Each Person
Each Person
Uninsured Motorist-PD
$
Each Accident
$
Vehicle
#2
Each Accident
$
Each Person
$
Each Accident
$
Each Accident
$
$
Each Accident
Each Accident
Personal Injury Protection
$
$
$
Each Person
Each Accident
Each Accident
$
$
Each Person
Each Person
Deductible
$
Each Accident
Deductible
Comprehensive Ded
Collision Ded
Towing & Labor
Trans Exp/Rental Reim
Customized Equipment
Other
Driver Description
Type of
Change
Driver Gender
Name
Marital
Status
Date of
Birth
Drivers
License #
Date
Licensed
Relationship to Named
Insured
SR-22
Filing
Remarks:
Applicant’s Signature
Date
Agent’s Signature
Date
<BW.NI1.S>
<BW.NI1.DS>
<BW.PA1.S>
<BW.PA1.DS>
PLEASE FAX POLICY CHANGE TO 1-844-843-7572.
Rated or
Excluded
Download policy change form
policy change form.pdf (PDF, 192.59 KB)
Download PDF
Share this file on social networks
Link to this page
Permanent link
Use the permanent link to the download page to share your document on Facebook, Twitter, LinkedIn, or directly with a contact by e-Mail, Messenger, Whatsapp, Line..
Short link
Use the short link to share your document on Twitter or by text message (SMS)
HTML Code
Copy the following HTML code to share your document on a Website or Blog
QR Code to this page

This file has been shared publicly by a user of PDF Archive.
Document ID: 0000598965.